
Here's the original article from JAMA Psychiatry that is making all the headlines recently. The authors suggest that their findings (if replicated) indicate that depressed patients should undergo a $2,000 PET scan test (which involves an intravenous injection of radioactive liquid) in order the decide whether they should receive Lexapro (an antidepressant) or CBT (a psychotherapy) as a first-line treatment for their depression.
The study randomly assigned 82 depressed patients (with the usual exclusion for patients with "current suicidal ideation requiring urgent clinical intervention") to either Lexapro (up to 20 mg qd) or CBT (16 sessions; twice weekly for the first 4 weeks, then weekly). After 12 weeks, 6 of the 30 (20.0%) Lexaprosiacs were still depressed, versus 9 of the 33 (27.3%) of the CBT'rs. (19 participants were excluded or terminated after randomization.)
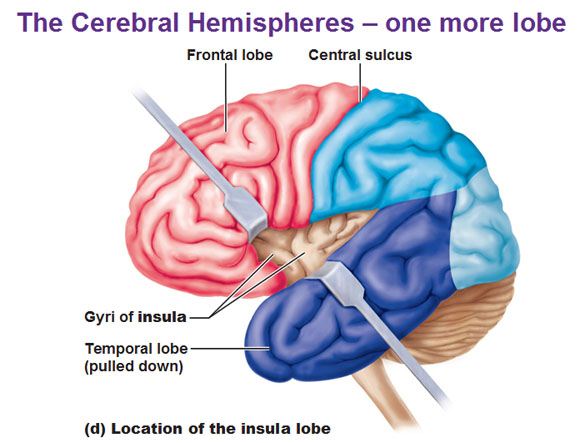
The researchers the did a two-way ANOVA [treatment (CBT or Lexapro) x outcome (remission or nonresponse)] to identify brain regions in the pre-treatment baseline PET scans that "predicted" (or rather, postdicted) treatment response. They found six such regions: right anterior insula, right inferior temporal cortex, left amgydala, left premotor cortex, right motor cortex, and precuneus. They found the strongest effect size for the insula and thus labelled it a "treatment-specific biomarker candidate."
Just a couple of comments:
1. The authors appropriately state that these findings require replication. This is because this study was a fishing expedition -- they had no idea, and no real reason to believe, that the metabolic rate of the right anterior insula would predict response to a specific treatment. They looked at dozens of brain regions, searching for "significant differences" between the groups and they found one -- just like you always will if you look at enough variables. What are the chances that these findings will be replicated by another group of researchers? Well, when is the last time you saw any study in neuroscience replicated by a second group of researchers? (It's pretty darn hard to replicate somebody else's random findings.)
2. Not having an initial hypothesis as to which brain regions might be involved is par for the course with these types of studies. This should be pretty shocking to anyone who ever got a B or higher in a psychology Research Methods course. The authors present very plausible-sounding reasons for why the right anterior insula is just so great at predicting treatment-specific response, but be aware that they would have come up with equally plausible-sounding reasons had the most significant effect been for the left premotor cortex or the precuneus (or the part of the brain that is involved in blink rate, if anyone knew what that was). Because human beings are very clever and creative, we can come up with plausible explanations for any random phenomenon (this is the pitfall of Freudian dream analysis -- AND of neuroscience).
3. It is really weird/lame that they found no main effect for remission. In other words, there was no brain region that predicted whether you would recover from your depressive episode in 12 weeks (regardless of which treatment you received). They are pretty silent about this non-result in their paper, although they sure seemed to think that they would find something.
4. It seems like the real question here is is not "Which brain region best predicts treatment outcome?" but rather "How do we match patients and treatments for the best results?" A future study should compare whether a clinician (or a psychological test, such as the MMPI-2) could perform the same task they are saying that the insula is doing (i.e., deciding which patients should get which treatment). And let's not lose sight of the fact that 76% of the patients recovered from their depressive episode despite being randomly assigned to either CBT or Lexapro, regardless of their personal preferences.
5. Would you rather have a clinical interview with a psychodiagnostician, complete a 90 minute True or False test, or have a radioactive i.v. followed by a PET scan that your insurance may or may not pay for?
6. My guess is that treatment-specific response has a lot to do with what kind of depression the patients had. We have known for a while now that people with dysthymia respond better to antidepressants than they do to psychotherapy, and people with chronic major depression respond better to combined therapy (AD meds + psychotherapy). How long the patients had been depressed was not noted in the insula study.
7. Any study that looks at psychotherapy efficacy and ignores therapeutic alliance (the strongest predictor of psychotherapy outcome) is courting worthlessness. Therapeutic alliance also influences response to antidepressant medications! If you don't like your psychiatrist (or if he doesn't like you), then you are less likely to get better.
8. Why do people persist in using the crappy little HAM-D as their only outcome measure of depression? Why not use the MMPI-2? If they had, we could have been able to tell the chronic depressives from the acute depressives (and which of the patients had hysteric defenses, paranoia, agitation, etc.).
For the best critiques of brain imaging studies (by an fMRI reseacher), I refer you to Neuroskeptic. As Neuroskeptic says, brain imaging "is a great way to approach neuroscientific questions. It’s a bad (and terribly expensive) way to do psychology." The new book, Brainwashed, by Scott Lilienfeld and Sally Satel, also promises to be well worth reading.
No comments:
Post a Comment
Note: Only a member of this blog may post a comment.